
Milk Consumption and Its Association with Dental Caries: Gender-Specific Insights from the Korea National Health and Nutrition Examination Survey (2013–2015)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview of the Study Design
2.2. Demographic Evaluation
2.3. Anthropometric Evaluation
2.4. Biochemical Analyses
2.5. Explanation of Metabolic Syndrome, Diabetes, Hypertension, Anemia, and Overview of Dental Caries and Oral Health Practices
2.6. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Górska-Warsewicz, H.; Rejman, K.; Laskowski, W.; Czeczotko, M. Milk and Dairy Products and Their Nutritional Contribution to the Average Polish Diet. Nutrients 2019, 11, 1771. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.D.; Jarvis, J.K.; McBean, L.D. The importance of meeting calcium needs with foods. J. Am. Coll. Nutr. 2001, 20, 168s–185s. [Google Scholar] [CrossRef]
- Thorning, T.K.; Raben, A.; Tholstrup, T.; Soedamah-Muthu, S.S.; Givens, I.; Astrup, A. Milk and dairy products: Good or bad for human health? An assessment of the totality of scientific evidence. Food Nutr. Res. 2016, 60, 32527. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Givens, D.I.; Heitmann, B.L. Association between dairy consumption and cardiovascular disease events, bone fracture and all-cause mortality. PLoS ONE 2022, 17, e0271168. [Google Scholar] [CrossRef]
- Salehiamin, M.; Toolee, H.; Azami, M.; Tafti, S.H.A.; Mojaverrostami, S.; Halimi, S.; Barakzai, S.; Sobhani, A.; Abbasi, Y. Chitosan Scaffold Containing Periostin Enhances Sternum Bone Healing and Decreases Serum Level of TNF-α and IL-6 after Sternotomy in Rat. Tissue Eng. Regen. Med. 2022, 19, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-E.; Jang, J.-H. Consumption of milk prevents dental caries by inhibiting sugar fermentation. Int. J. Clin. Prev. Dent. 2017, 13, 31–37. [Google Scholar] [CrossRef]
- Virkkala, V.F.; Eloranta, A.-M.; Suominen, A.L.; Vierola, A.; Ikävalko, T.; Väistö, J.; Mikkonen, S.; Methuen, M.; Schwab, U.; Viljakainen, H.T.; et al. Associations of diet quality, food consumption, eating frequency and eating behaviour with dental caries experience in Finnish children: A 2-year longitudinal study. Br. J. Nutr. 2022, 129, 1415–1425. [Google Scholar] [CrossRef]
- Palacios, C.; Rivas-Tumanyan, S.; Morou-Bermúdez, E.; Colon, A.M.; Torres, R.Y.; Elías-Boneta, A.R. Association between Type, Amount, and Pattern of Carbohydrate Consumption with Dental Caries in 12-Year-Olds in Puerto Rico. Caries Res. 2016, 50, 560–570. [Google Scholar] [CrossRef]
- Tan, S.F.; Tong, H.J.; Lin, X.Y.; Mok, B.; Hong, C.H. The cariogenicity of commercial infant formulas: A systematic review. Eur. Arch. Paediatr. Dent. 2016, 17, 145–156. [Google Scholar] [CrossRef]
- Johansson, I.; Esberg, A.; Eriksson, L.; Haworth, S.; Holgerson, P.L. Self-reported bovine milk intake is associated with oral microbiota composition. PLoS ONE 2018, 13, e0193504. [Google Scholar] [CrossRef]
- Marshall, T.A.; Levy, S.M.; Broffitt, B.; Warren, J.J.; Eichenberger-Gilmore, J.M.; Burns, T.L.; Stumbo, P.J. Dental caries and beverage consumption in young children. Pediatrics 2003, 112, e184–e191. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.R.; Park, Y.K.; Lim, H.S. Breastfeeding Duration Is Associated with the Risk of Tooth Loss, Chewing Difficulty, and Undernutrition among Older Korean Women: Results of the Korea National Health and Nutrition Examination Survey (KNHANES) 2013–2015. Nutrients 2023, 15, 5024. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Kim, E.-J.; Choi, Y.-K. Allergic rhinitis and periodontitis among Korean adults: Results from a nationwide population-based study (2013–2015). BMC Ear. Nose Throat Disord 2018, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Rha, E.Y.; Kim, H.J.; Han, K.; Park, Y.; Yoo, G. Gender-specific relationship between alcohol consumption and injury in the South Korean adults: A nationwide cross-sectional study. Medicine 2017, 96, e5385. [Google Scholar] [CrossRef] [PubMed]
- Hong, S. Association of Relative Handgrip Strength and Metabolic Syndrome in Korean Older Adults: Korea National Health and Nutrition Examination Survey VII-1. J. Obes. Metab. Syndr. 2019, 28, 53–60. [Google Scholar] [CrossRef]
- Lee, W.; Han, E.; Choi, J. Association of Participation in Disease Management Programs and Health-Related Quality of Life in Korean Population: Results from the Korea National Health and Nutrition Examination Survey IV and V (2007–2012). J. Prim. Care Community Health 2021, 12, 21501327211012185. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.H.; Han, K.; Kim, D.H.; Park, Y.G.; Cho, K.H.; Choi, Y.S.; Nam, G.E. Association of Urinary Sodium Excretion with Insulin Resistance in Korean Adolescents: Results from the Korea National Health and Nutrition Examination Survey 2009–2010. Medicine 2016, 95, e3447. [Google Scholar] [CrossRef]
- Woo, G.-J.; Lee, H.-R.; Kim, Y.; Kim, H.-J.; Park, D.-Y.; Kim, J.-B.; Oh, K.-W.; Choi, Y.-H. Data resource profile: Oral examination of the Korea National Health and Nutrition Examination Survey. J. Korean Acad. Oral. Health 2018, 42, 101–108. [Google Scholar] [CrossRef]
- Oh, K.; Kim, Y.; Kweon, S.; Kim, S.; Yun, S.; Park, S.; Lee, Y.-K.; Kim, Y.; Park, O.; Jeong, E.K. Korea National Health and Nutrition Examination Survey, 20th anniversary: Accomplishments and future directions. Epidemiol. Health 2021, 43, e2021025. [Google Scholar] [CrossRef]
- Han, K.; Park, J.B. Association between oral health behavior and periodontal disease among Korean adults: The Korea national health and nutrition examination survey. Medicine 2017, 96, e6176. [Google Scholar] [CrossRef] [PubMed]
- Al-Jobair, A.; Khounganian, R. Evaluating the cariogenic potential of flavored milk: An experimental study using rat model. J. Contemp. Dent. Pract. 2015, 16, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.S.; Nugent, Z.J.; Rudolf, M.C.J.; Sahota, P. Dietary patterns, toothbrushing habits and caries experience of schoolchildren in West Yorkshire, England. Community Dent. Health 2007, 24, 82–87. [Google Scholar] [PubMed]
- Stösser, L.; Kneist, S.; Grosser, W. The effects of non-fluoridated and fluoridated milk on experimental caries in rats. Adv. Dent. Res. 1995, 9, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-B.; Kim, I.; Lee, W.; Kim, H. Evaluation of the regenerative capacity of stem cells combined with bone graft material and collagen matrix using a rabbit calvarial defect model. J. Periodontal Implant. Sci. 2023, 53, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Ricomini Filho, A.P.; de Assis, A.C.M.; Costa Oliveira, B.E.; Cury, J.A. Cariogenic Potential of Human and Bovine Milk on Enamel Demineralization. Caries Res. 2021, 55, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Peres, R.C.R.; Coppi, L.C.; Franco, E.M.; Volpato, M.C.; Groppo, F.C.; Rosalen, P.L. Cariogenicity of different types of milk: An experimental study using animal model. Braz. Dent. J. 2002, 13, 27–32. [Google Scholar] [PubMed]
- Sezer, B.; Giritlioğlu, B.; Sıddıkoğlu, D.; Lussi, A.; Kargül, B. Relationship between erosive tooth wear and possible etiological factors among dental students. Clin. Oral Investig. 2022, 26, 4229–4238. [Google Scholar] [CrossRef]
- Bánóczy, J.; Zimmermann, P.; Pintér, A.; Hadas, E.; Bruszt, V. Effect of fluoridated milk on caries: 3-year results. Community Dent. Oral Epidemiol. 1983, 11, 81–85. [Google Scholar] [CrossRef]
- Tinanoff, N. Association of diet with dental caries in preschool children. Dent. Clin. N. Am. 2005, 49, 725–737. [Google Scholar] [CrossRef]
- Amer, S.; Kateeb, E. Factors related to dietary habits, energy drink consumption, and physical activity in marginalized Palestinian schools: A cross-sectional study. Health Promot. Perspect. 2021, 11, 329–336. [Google Scholar] [CrossRef]
- Lukacs, J.R.; Largaespada, L.L. Explaining sex differences in dental caries prevalence: Saliva, hormones, and ”life-history” etiologies. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2006, 18, 540–555. [Google Scholar] [CrossRef]
- Ortiz, S.; Herrman, E.; Lyashenko, C.; Purcell, A.; Raslan, K.; Khor, B.; Snow, M.; Forsyth, A.; Choi, D.; Maier, T.; et al. Sex-specific differences in the salivary microbiome of caries-active children. J. Oral Microbiol. 2019, 11, 1653124. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, M.; Vieira, A.R. Explaining gender differences in caries: A multifactorial approach to a multifactorial disease. Int. J. Dent. 2010, 2010, 649643. [Google Scholar] [CrossRef] [PubMed]
- Pryzhkova, M.V.; Boers, R.; Jordan, P.W. Modeling Human Gonad Development in Organoids. Tissue Eng. Regen. Med. 2022, 19, 1185–1206. [Google Scholar] [CrossRef]
- Niu, J.; Feng, F.; Zhang, S.; Zhu, Y.; Song, R.; Li, J.; Zhang, M. Thrombospondin-2 Couples Pressure-Promoted Chondrogenesis through NF-κB Signaling. Tissue Eng. Regen. Med. 2023, 20, 753–766. [Google Scholar] [CrossRef]
- Costa, S.M.; Vasconcelos, M.; A Haddad, J.P.; Abreu, M.H.N. The severity of dental caries in adults aged 35 to 44 years residing in the metropolitan area of a large city in Brazil: A cross-sectional study. BMC Oral. Health 2012, 12, 25. [Google Scholar] [CrossRef]
- Shetty, J.; Hegde, M.; Devadiga, D.; D’Souza, N. Prevalence of root caries in Indian population-a systematic review and meta-analysis. Evid. Based Dent. 2023, 24, 192. [Google Scholar] [CrossRef] [PubMed]
- Houston, W.J. The analysis of errors in orthodontic measurements. Am. J. Orthod. 1983, 83, 382–390. [Google Scholar] [CrossRef]
- Chung, W.; Lim, S.-J.; Lee, S.; Kim, R.; Kim, J. Gender-specific interactions between education and income in relation to obesity: A cross-sectional analysis of the Fifth Korea National Health and Nutrition Examination Survey (KNHANES V). BMJ Open 2017, 7, e014276. [Google Scholar] [CrossRef]
- Han, K.; Ko, Y.; Park, Y.G.; Park, J.B. Associations Between the Periodontal Disease in Women Before Menopause and Menstrual Cycle Irregularity: The 2010-2012 Korea National Health and Nutrition Examination Survey. Medicine 2016, 95, e2791. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Lee, E.; Park, J.B. Evaluation of the associations between immunoglobulin E levels and the number of natural teeth. J. Formos. Med. Assoc. Taiwan Yi Zhi 2018, 117, 605–612. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Dental Caries | ||||||
|---|---|---|---|---|---|---|
| Yes | No | p-Value * | Yes | No | p-Value * | |
| Male (n = 6656) | Female (n = 8925) | |||||
| n = 5791 | n = 865 | n = 8266 | n = 695 | |||
| Age (years) | 44.97 ± 0.49 | 45.80 ± 1.28 | 0.5192 | 46.90 ± 0.51 | 51.25 ± 1.83 | 0.0168 |
| Height (cm) | 170.98 ± 0.20 | 169.95 ± 0.46 | 0.0395 | 157.51 ± 0.18 | 155.88 ± 0.59 | 0.0056 |
| Weight (kg) | 71.24 ± 0.33 | 70.85 ± 0.78 | 0.6445 | 57.71 ± 0.22 | 55.71 ± 0.70 | 0.0070 |
| BMI (kg/m2) | 24.32 ± 0.10 | 24.46 ± 0.22 | 0.5892 | 23.28 ± 0.09 | 22.92 ± 0.29 | 0.2046 |
| Waist circumference (cm) | 83.94 ± 0.29 | 84.44 ± 0.68 | 0.4762 | 77.30 ± 0.31 | 77.24 ± 0.90 | 0.9518 |
| Systolic pressure (mmHg) | 119.02 ± 0.42 | 119.66 ± 0.94 | 0.5252 | 114.21 ± 0.50 | 119.79 ± 1.88 | 0.0026 |
| Diastolic pressure (mmHg) | 77.71 ± 0.34 | 77.49 ± 0.80 | 0.7931 | 72.66 ± 0.30 | 72.23 ± 0.87 | 0.6338 |
| Fasting glucose (mmol/dL) | 100.44 ± 0.63 | 98.95 ± 1.21 | 0.2720 | 96.77 ± 0.57 | 95.90 ± 1.39 | 0.5479 |
| HbA1c (%) | 5.87 ± 0.02 | 5.88 ± 0.05 | 0.8314 | 5.81 ± 0.02 | 5.83 ± 0.06 | 0.7923 |
| Total cholesterol (mmol/dL) | 186.72 ± 1.15 | 185.46 ± 2.77 | 0.6727 | 188.47 ± 0.92 | 192.20 ± 3.23 | 0.2652 |
| High density lipoprotein (mg/dL) | 47.62 ± 0.32 | 46.94 ± 0.74 | 0.3613 | 54.06 ± 0.27 | 55.33 ± 1.09 | 0.2459 |
| Triglycerides (mmol/dL) | 159.95 ± 3.87 | 167.04 ± 9.96 | 0.4995 | 112.95 ± 2.06 | 115.18 ± 6.38 | 0.7262 |
| Creatinine (mg/dL) | 0.98 ± 0.01 | 1.07 ± 0.09 | 0.3529 | 0.73 ± 0.01 | 0.73 ± 0.01 | 0.5449 |
| WBC count (109/L) | 6.48 ± 0.05 | 6.51 ± 0.11 | 0.8278 | 5.74 ± 0.05 | 5.75 ± 0.15 | 0.9827 |
| Vitamin D (ng/mL) | 17.67 ± 0.35 | 17.22 ± 0.73 | 0.5413 | 15.98 ± 0.31 | 16.83 ± 1.44 | 0.5567 |
| Calcium intake (mg/day) | 567.63 ± 8.34 | 568.29 ± 23.38 | 0.9783 | 493.82 ± 6.51 | 488.30 ± 22.75 | 0.8142 |
| Hypertension | ||||||
| No | 72.5 | 11.3 | 0.1259 | 76.6 | 5.8 | 0.0610 |
| Yes | 13.5 | 2.8 | 15.9 | 1.7 | ||
| Diabetes mellitus | ||||||
| Normal | 55.3 | 8.6 | 0.9883 | 69.4 | 5.6 | 0.1256 |
| Impaired fasting glucose | 21.5 | 3.3 | 16.2 | 0.8 | ||
| Diabetes mellitus | 9.8 | 1.6 | 7.4 | 0.7 | ||
| Anemia | ||||||
| No | 83.7 | 13.4 | 0.9504 | 81.5 | 6.2 | 0.6748 |
| Yes | 2.5 | 0.4 | 11.4 | 1.0 | ||
| Metabolic syndrome | ||||||
| Yes | 57.5 | 9.9 | 0.8791 | 63.0 | 5.1 | 0.6939 |
| No | 27.7 | 4.9 | 29.4 | 2.5 | ||
| Housing (region) | ||||||
| City(-si) | 39.0 | 6.6 | 0.7653 | 45.2 | 4.1 | 0.2007 |
| Province(-do) | 46.9 | 7.5 | 47.3 | 3.5 | ||
| Income level | ||||||
| High | 26.8 | 3.9 | 0.4344 | 26.8 | 1.8 | 0.1992 |
| Low | 59.3 | 10.0 | 65.7 | 5.7 | ||
| Education | ||||||
| Lower than high school graduate | 17.1 | 3.2 | 0.3308 | 30.0 | 2.9 | 0.1547 |
| High school graduate or higher | 68.8 | 10.9 | 62.5 | 4.6 | ||
| Occupation classification | ||||||
| Administrators | 13.2 | 2.0 | 0.0641 | 11.2 | 0.6 | 0.1851 |
| Professionals and allied workers | 11.2 | 1.1 | 7.9 | 0.6 | ||
| Office workers | 11.8 | 1.9 | 13.8 | 0.7 | ||
| Service workers | 4.2 | 0.4 | 2.0 | 0.3 | ||
| Sales | 17.3 | 2.6 | 2.1 | 0.2 | ||
| Agriculture, forestry and fisheries skilled workers | 5.8 | 1.5 | 8.8 | 0.9 | ||
| Skilled trades and related workers | 22.5 | 4.4 | 46.8 | 4.2 | ||
| AUDIT score | ||||||
| 0–7, 8–14 | 65.7 | 11.1 | 0.7081 | 89.9 | 7.0 | 0.1211 |
| 15–19, ≥20 | 20.0 | 3.2 | 3.0 | 0.1 | ||
| Heavy drinking | ||||||
| No | 26.7 | 4.5 | 0.8238 | 63.3 | 5.9 | 0.0136 |
| Yes | 59.2 | 9.6 | 29.2 | 1.6 | ||
| Frequency of drinking in one year | ||||||
| Less than once a month | 22.1 | 3.4 | 0.8572 | 53.3 | 4.8 | 0.1166 |
| One to four times a month | 34.2 | 5.5 | 29.5 | 2.2 | ||
| Two or more times a week | 29.7 | 5.1 | 9.7 | 0.5 | ||
| Smoking | ||||||
| Nonsmoker | 35.2 | 5.9 | 0.0592 | 5.7 | 0.5 | 0.4326 |
| Ex-smoker | 28.7 | 5.5 | 4.7 | 0.2 | ||
| Current smoker | 22.0 | 2.7 | 82.2 | 6.7 | ||
| Regular physical exercise (average number of days per week) | 3.15 ± 0.04 | 3.13 ± 0.12 | 0.8320 | 2.76 ± 0.03 | 2.48 ± 0.09 | 0.0035 |
| Toothbrushing yesterday | ||||||
| No | 0.5 | 1.2 | 0.0249 | 0.2 | 1.0 | 0.0849 |
| Yes | 13.6 | 84.8 | 7.2 | 91.5 | ||
| Frequency of milk consumption | ||||||
| Low | 67.8 | 11.1 | 0.1419 | 69.3 | 5.2 | 0.3054 |
| High | 18.9 | 2.2 | 24.1 | 1.4 | ||
| Amount of milk consumption | ||||||
| Low | 22.4 | 4.0 | 0.2719 | 27.8 | 2.3 | 0.1906 |
| High | 64.3 | 9.3 | 65.7 | 4.2 | ||
| Types of milk | ||||||
| Whole milk | 62.7 | 9.5 | 0.3458 | 58.3 | 4.0 | 0.8672 |
| Low-fat milk | 12.9 | 1.3 | 22.5 | 1.5 | ||
| Similar (whole/low-fat) | 11.7 | 2.0 | 12.8 | 1.0 | ||
| Variable | Level | Estimate | Standard Error | Wald Chi-Square | p-Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|---|---|---|
| Milk Amount | Low | |||||||
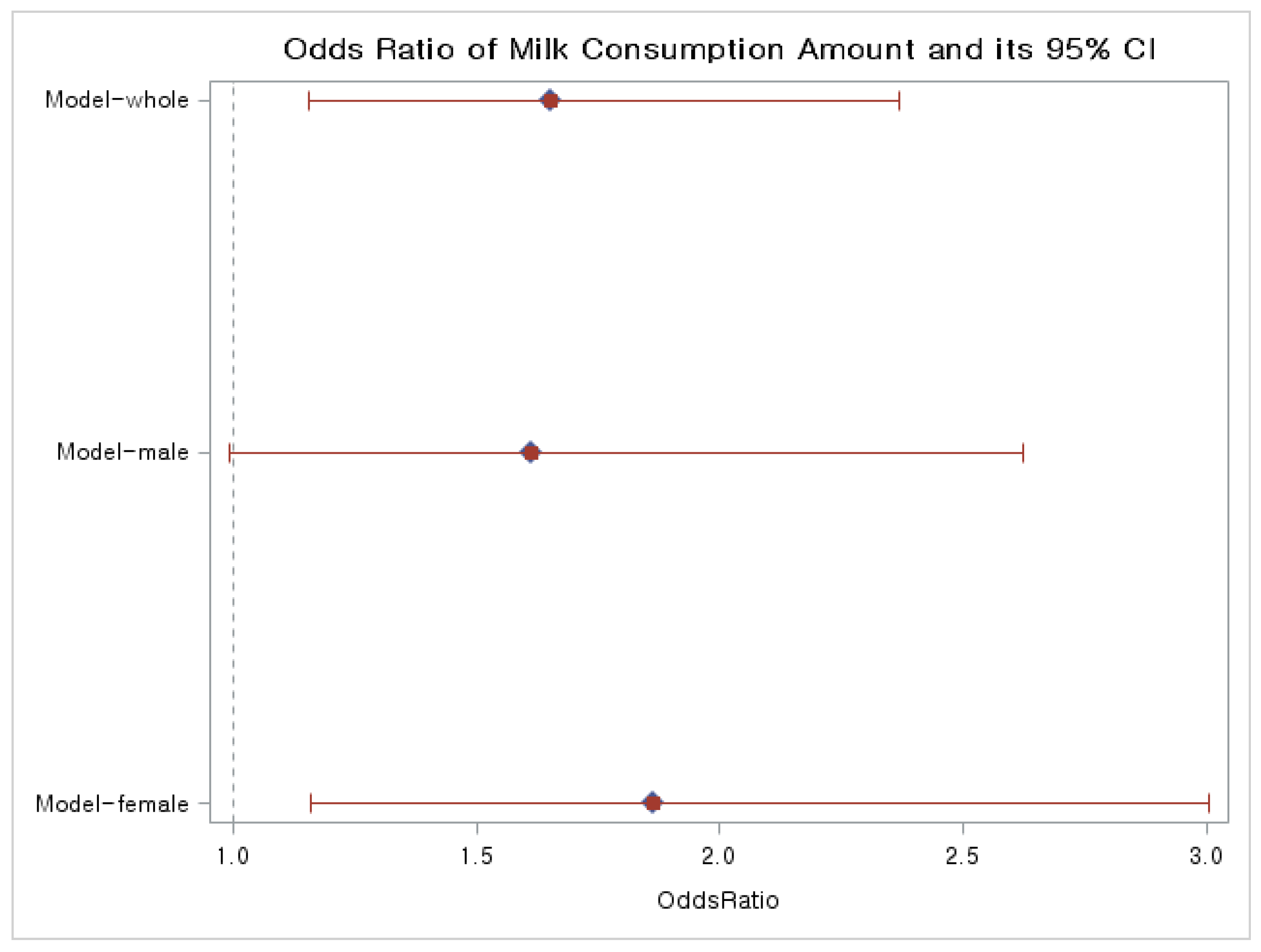
| High | 0.503 | 0.1838 | 7.475 | 0.006 | 1.653 | 1.153 | 2.370 | |
| Age | 0.003 | 0.010 | 0.111 | 0.739 | 1.003 | 0.984 | 1.022 | |
| Gender | Female | |||||||
| Male | −0.697 | 0.245 | 8.131 | 0.004 | 0.498 | 0.308 | 0.804 | |
| Smoking | Current | |||||||
| Ex- | −0.174 | 0.238 | 0.533 | 0.466 | 0.841 | 0.528 | 1.340 | |
| Non- | 0.225 | 0.274 | 0.679 | 0.410 | 1.253 | 0.733 | 2.141 | |
| Drinking | Non- | |||||||
| Light-medium | −0.193 | 0.216 | 0.794 | 0.373 | 0.825 | 0.540 | 1.260 | |
| Heavy | 0.021 | 0.260 | 0.007 | 0.936 | 1.021 | 0.614 | 1.699 | |
| BMI | 0.004 | 0.032 | 0.014 | 0.905 | 1.004 | 0.943 | 1.068 | |
| Regular physical exercise (average number of days per week) | 0.003 | 0.064 | 0.002 | 0.965 | 1.003 | 0.885 | 1.136 | |
| Education | Lower than high school graduate | |||||||
| High school graduate or higher | −0.251 | 0.266 | 0.892 | 0.345 | 0.778 | 0.462 | 1.310 | |
| Income | Low | |||||||
| High | 0.101 | 0.192 | 0.275 | 0.600 | 1.106 | 0.759 | 1.613 | |
| Region | City(-si) | |||||||
| Province(-do) | 0.044 | 0.184 | 0.057 | 0.812 | 1.045 | 0.728 | 1.499 | |
| Diabetes mellitus | Normal | |||||||
| Impaired fasting glucose | 0.486 | 0.236 | 4.247 | 0.039 | 1.626 | 1.024 | 2.582 | |
| Diabetes mellitus | 0.404 | 0.333 | 1.467 | 0.226 | 1.497 | 0.779 | 2.877 | |
| Hypertension | Normal | |||||||
| High | −0.355 | 0.251 | 1.998 | 0.158 | 0.701 | 0.428 | 1.147 | |
| WBC count | 0.020 | 0.058 | 0.113 | 0.737 | 1.020 | 0.910 | 1.143 | |
| Metabolic syndrome | No | |||||||
| Yes | −0.073 | 0.213 | 0.116 | 0.733 | 0.930 | 0.612 | 1.413 | |
| Toothbrushing yesterday | No | |||||||
| Yes | −0.435 | 1.044 | 0.174 | 0.677 | 0.647 | 0.084 | 5.006 | |
| Variable | Level | Estimate | Standard Error | Wald Chi-Square | p-Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|---|---|---|
| Milk Amount | Low | |||||||
| High | 0.478 | 0.2485 | 3.699 | 0.054 | 1.613 | 0.991 | 2.625 | |
| Age | 0.021 | 0.012 | 2.966 | 0.085 | 1.022 | 0.997 | 1.047 | |
| Smoking | Current | |||||||
| Ex- | −0.240 | 0.260 | 0.849 | 0.357 | 0.787 | 0.472 | 1.310 | |
| Non- | 0.380 | 0.330 | 1.326 | 0.250 | 1.462 | 0.766 | 2.789 | |
| Drinking | Non- | |||||||
| Light-medium | 0.123 | 0.279 | 0.195 | 0.659 | 1.131 | 0.655 | 1.953 | |
| Heavy | 0.112 | 0.301 | 0.138 | 0.710 | 1.118 | 0.620 | 2.017 | |
| BMI | −0.006 | 0.041 | 0.022 | 0.882 | 0.994 | 0.918 | 1.076 | |
| Regular physical exercise (average number of days per week) | −0.030 | 0.082 | 0.136 | 0.712 | 0.970 | 0.827 | 1.139 | |
| Education | Lower than high school graduate | |||||||
| High school graduate or higher | 0.090 | 0.344 | 0.068 | 0.794 | 1.094 | 0.557 | 2.149 | |
| Income | Low | |||||||
| High | −0.063 | 0.228 | 0.076 | 0.783 | 0.939 | 0.601 | 1.468 | |
| Region | City(-si) | |||||||
| Province(-do) | −0.095 | 0.226 | 0.176 | 0.675 | 0.910 | 0.584 | 1.416 | |
| Diabetes | Normal | |||||||
| Impaired fasting glucose | 0.269 | 0.271 | 0.981 | 0.322 | 1.308 | 0.769 | 2.227 | |
| Diabetes mellitus | 0.193 | 0.402 | 0.231 | 0.631 | 1.213 | 0.552 | 2.665 | |
| Hypertension | Normal | |||||||
| High | −0.557 | 0.319 | 3.046 | 0.081 | 0.573 | 0.306 | 1.071 | |
| WBC count | 0.005 | 0.078 | 0.005 | 0.944 | 1.005 | 0.864 | 1.170 | |
| Metabolic syndrome | No | |||||||
| Yes | 0.079 | 0.283 | 0.078 | 0.780 | 1.082 | 0.622 | 1.883 | |
| Toothbrushing yesterday | No | |||||||
| Yes | −12.178 | 0.563 | 468.305 | <.0001 | <0.001 | <0.001 | <0.001 | |
| Variable | Level | Estimate | Standard Error | Wald Chi-Square | p-Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|---|---|---|
| Milk Amount | Low | |||||||
| High | 0.623 | 0.2436 | 6.542 | 0.011 | 1.865 | 1.157 | 3.006 | |
| Age | −0.038 | 0.019 | 4.108 | 0.043 | 0.963 | 0.928 | 0.999 | |
| Smoking | Current | |||||||
| Ex- | 0.456 | 0.825 | 0.305 | 0.581 | 1.577 | 0.313 | 7.950 | |
| Non- | 0.376 | 0.655 | 0.329 | 0.566 | 1.456 | 0.404 | 5.251 | |
| Drinking | Non- | |||||||
| Light-medium | −0.760 | 0.309 | 6.057 | 0.014 | 0.468 | 0.255 | 0.857 | |
| Heavy | 0.900 | 0.636 | 2.001 | 0.157 | 2.460 | 0.707 | 8.562 | |
| BMI | 0.022 | 0.050 | 0.194 | 0.660 | 1.022 | 0.927 | 1.127 | |
| Regular physical exercise (average number of days per week) | 0.148 | 0.101 | 2.124 | 0.145 | 1.003 | 0.885 | 1.136 | |
| Education | Lower than high school graduate | |||||||
| High school graduate or higher | −0.954 | 0.355 | 7.213 | 0.007 | 1.159 | 0.950 | 1.413 | |
| Income | Low | |||||||
| High | 0.605 | 0.343 | 3.109 | 0.078 | 1.831 | 0.935 | 3.588 | |
| Region | City(-si) | |||||||
| Province(-do) | 0.313 | 0.277 | 1.274 | 0.259 | 1.367 | 0.794 | 2.352 | |
| Diabetes mellitus | Normal | |||||||
| Impaired fasting glucose | 1.113 | 0.398 | 7.824 | 0.005 | 3.042 | 1.395 | 6.634 | |
| Diabetes mellitus | 0.784 | 0.596 | 1.730 | 0.189 | 2.191 | 0.681 | 7.051 | |
| Hypertension | Normal | |||||||
| High | 0.201 | 0.413 | 0.237 | 0.626 | 1.223 | 0.544 | 2.747 | |
| WBC | 0.049 | 0.082 | 0.357 | 0.550 | 1.050 | 0.895 | 1.232 | |
| Metabolic syndrome | No | |||||||
| Yes | −0.253 | 0.344 | 0.543 | 0.461 | 0.776 | 0.396 | 1.523 | |
| Toothbrushing yesterday | No | |||||||
| Yes | 1.009 | 1.056 | 0.913 | 0.339 | 2.742 | 0.346 | 21.718 | |
| Gender | Dental Caries | Amount of Milk Consumption | p-Value | |
|---|---|---|---|---|
| Low | High | |||
| Male | No | 53 (15.1) | 116 (12.7) | 0.2719 |
| Yes | 332 (84.9) | 834 (87.3) | ||
| Female | No | 50 (7.79) | 75 (6.0) | 0.1906 |
| Yes | 572 (92.39) | 1300 (94.0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Min, E.J.; Park, E.; Park, J.-B. Milk Consumption and Its Association with Dental Caries: Gender-Specific Insights from the Korea National Health and Nutrition Examination Survey (2013–2015). Medicina 2024, 60, 967. https://doi.org/10.3390/medicina60060967
Min EJ, Park E, Park J-B. Milk Consumption and Its Association with Dental Caries: Gender-Specific Insights from the Korea National Health and Nutrition Examination Survey (2013–2015). Medicina. 2024; 60(6):967. https://doi.org/10.3390/medicina60060967
Chicago/Turabian StyleMin, Eun Jeong, EunKyung Park, and Jun-Beom Park. 2024. "Milk Consumption and Its Association with Dental Caries: Gender-Specific Insights from the Korea National Health and Nutrition Examination Survey (2013–2015)" Medicina 60, no. 6: 967. https://doi.org/10.3390/medicina60060967